11
Jun

Anil Jauhri

New Delhi | Thursday | June 11, 2026
My first encounter with healthcare accreditation came in late 2005 when, as head of management systems certification at BIS, I learned of the establishment of the National Accreditation Board for Hospitals and Healthcare Providers (NABH) within the Quality Council of India (QCI) and the launch of India's first hospital accreditation standard.
The concept intrigued me. In the ISO world, accreditation is understood as an attestation of competence of conformity assessment bodies such as testing laboratories, inspection bodies and certification bodies. Healthcare accreditation appeared to be something different.
Soon after, in January 2006, I joined QCI as Adviser. Curious to understand this emerging field, I requested Dr G. J. Gyani, then Secretary General of QCI and founder of NABH, to allow me to attend one of its programmes. He readily agreed. At a session in Pune, I listened to an outstanding lecture on quality by Dr Y. P. Bhatia, one of the pioneers of healthcare quality in India.
That experience helped me understand the essential distinction. Healthcare accreditation, much like accreditation in education, focuses primarily on processes and systems rather than on competence in the ISO sense. In many respects, it resembles process certification.
Over the years, I watched NABH grow impressively. It secured endorsement from the International Society for Quality in Health Care (ISQua), achieving international recognition. While serving as CEO of the National Accreditation Board for Certification Bodies (NABCB), I occasionally attended NABH Board meetings and observed its progress from close quarters.
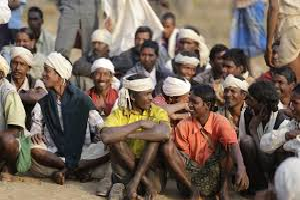
Even so, my engagement with healthcare quality remained limited. I often argued that India needed to implement minimum standards for healthcare establishments, as envisaged under the Clinical Establishments Act, to improve quality at scale. Accreditation certainly showcases excellence, but given India's vast healthcare ecosystem, accreditation alone cannot address the quality needs of the entire sector.
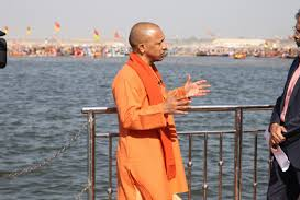
My interest in the subject deepened considerably when the Ministry of Ayush invited me in January 2025 to chair a Working Group tasked with identifying Ayush products and services that meet global standards. The exercise culminated in the launch of the Ayush Quality Mark by the Prime Minister in December 2025.
During this work, I took a closer look at healthcare and education accreditation systems and discovered something that surprised me: the inherent conflict of interest permitted in healthcare accreditation.
Under the ISQua External Evaluation Association's Guidelines and Standards for External Evaluation Organisations (5th Edition, Version 1.1, March 2022), Criterion 1.7 requires only that there be a defined separation between external evaluation activities and consultancy services, and that this separation be communicated to stakeholders.
In other words, the same legal entity may provide both consultancy and accreditation, provided it maintains an internal separation between the two activities.
This approach differs fundamentally from the principles embedded in ISO-based accreditation and certification systems.
ISO 17011, the international standard for accreditation bodies, explicitly prohibits accreditation bodies and any part of the same legal entity from providing consultancy services. Similarly, ISO 17021-1, which underpins management systems certification worldwide, prohibits certification bodies and related entities from offering management system consultancy. ISO 17065, governing product and process certification, contains comparable restrictions.
These provisions are based on a simple and universally accepted principle: one should not audit one's own work.
Healthcare accreditation systems that permit consultancy and accreditation within the same legal entity may argue that different individuals perform the two functions. Yet this does not eliminate the underlying conflict. Internal separation is not the same as institutional independence. The issue is not merely actual conflict of interest but also the perception of conflict, which can be equally damaging to credibility.
This concern led the Ayush Working Group to prescribe additional requirements. We decided that accreditation bodies operating under the Ayush Quality Mark programme should not provide consultancy services. This may render some well-known accreditation organisations ineligible unless they modify their practices, but integrity, independence and impartiality must take precedence.
The issue extends beyond organisations themselves.
If an accreditation body is prohibited from consulting, should its personnel be allowed to do so independently? In my view, the answer should be no. Yet even ISO-based systems have weaknesses in this regard. Consultants are often empanelled as auditors, creating a marketplace where advisory and assessment roles overlap. The same concern naturally applies to healthcare accreditation systems.
Other potential conflicts also deserve attention.
Can an accreditation body owned by a hospital chain or healthcare consulting organisation truly be perceived as independent? Can an accreditation body remain impartial if it approves or empanels consultants who operate in the same market?
Such arrangements create incentives that may compromise objectivity. When assessors encounter an organisation that has been advised by an approved consultant, there may be an unconscious reluctance to identify significant deficiencies. Doing so could raise questions not only about the consultant's competence but also about the accreditation body's own approval processes.
For this reason, accreditation bodies should maintain as much distance as possible from consultancy activities and consulting networks.
This does not mean they have no role in capacity building. Since accreditation bodies develop and own accreditation programmes, they are often best placed to explain standards and expectations. Public training programmes on standards can therefore be entirely appropriate. However, they should avoid becoming providers of consultancy services aimed at helping organisations achieve accreditation.
A better solution would be to strengthen independent skills and training ecosystems. In India, sector skill councils already exist in many domains, including healthcare. Bodies such as the Healthcare Sector Skill Council could independently certify professionals and training programmes to meet sectoral needs, while accreditation bodies concentrate exclusively on conducting impartial assessments.
The distinction may appear subtle, but it is crucial. Accreditation derives its value from trust. Once doubts arise about independence or impartiality, the credibility of the entire system is weakened.
Healthcare is an especially sensitive sector because accreditation decisions influence patient confidence, institutional reputation and, ultimately, public welfare. The standards governing accreditation must therefore be held to the highest levels of integrity.
The Ayush Quality Mark programme has attempted to establish such a benchmark by prescribing clear safeguards against actual and perceived conflicts of interest. Whether these principles gain wider acceptance remains to be seen, but they reflect a simple conviction: independence and impartiality are not optional attributes of accreditation. They are its foundation.
The author is former CEO, National Accreditation Board for Certification Bodies, Quality Council of India


About Silence And Accountability
29 Jul 2026




When women in uniform speak, society must listen
29 Jun 2026







CRICKET : IS POLITICS COLOURING SELECTIONS?
30 May 2026



No chance of cockroach Mukt Universe
18 May 2026

T20 SELECTIONS GET TOUGHER
17 May 2026
Election Verdict : What Ails The Opposition
10 May 2026

नोएडा में मज़दूरों पर लाठियाँ और झूठ
10 May 2026

चुनावी फ़ैसला : विपक्ष की कमजोरी क्या है
10 May 2026


THE FALLACY OF ONE NATION ONE STANDARD
24 Apr 2026
Gulf War poses serious threat to Indian Economy
24 Apr 2026
MY Love Affair With William Shakespeare
24 Apr 2026
एक और कठिन लड़ाई में उलझे हुए राष्ट्रपति ट्रंप
13 Apr 2026


LOOKING BACK AT T20 world Cup
10 Apr 2026



LESSONS FROM CHINTAN SHIVIR ON MEDICAL DEVICES
30 Mar 2026
रेजीम तो बदलेगा, मगर ईरान में नहीं—अमेरिका में!
28 Mar 2026

ट्रम्प की धमकी के जवाब में ईरान का धमाका
25 Mar 2026

एक सहानुभूतिपूर्ण जीत, आनंदित होने का समय
14 Mar 2026


डॉ. जे.एस. यादव: द मैन एंड हिज मिशन
14 Mar 2026
भ्रष्टाचार के खिलाफ भाजपा: मिथक और वास्तविकता
14 Mar 2026



Dr J.S. Yadav: The Man And His Mission
12 Mar 2026
An Empathic Win, A Time To Rejoice
12 Mar 2026

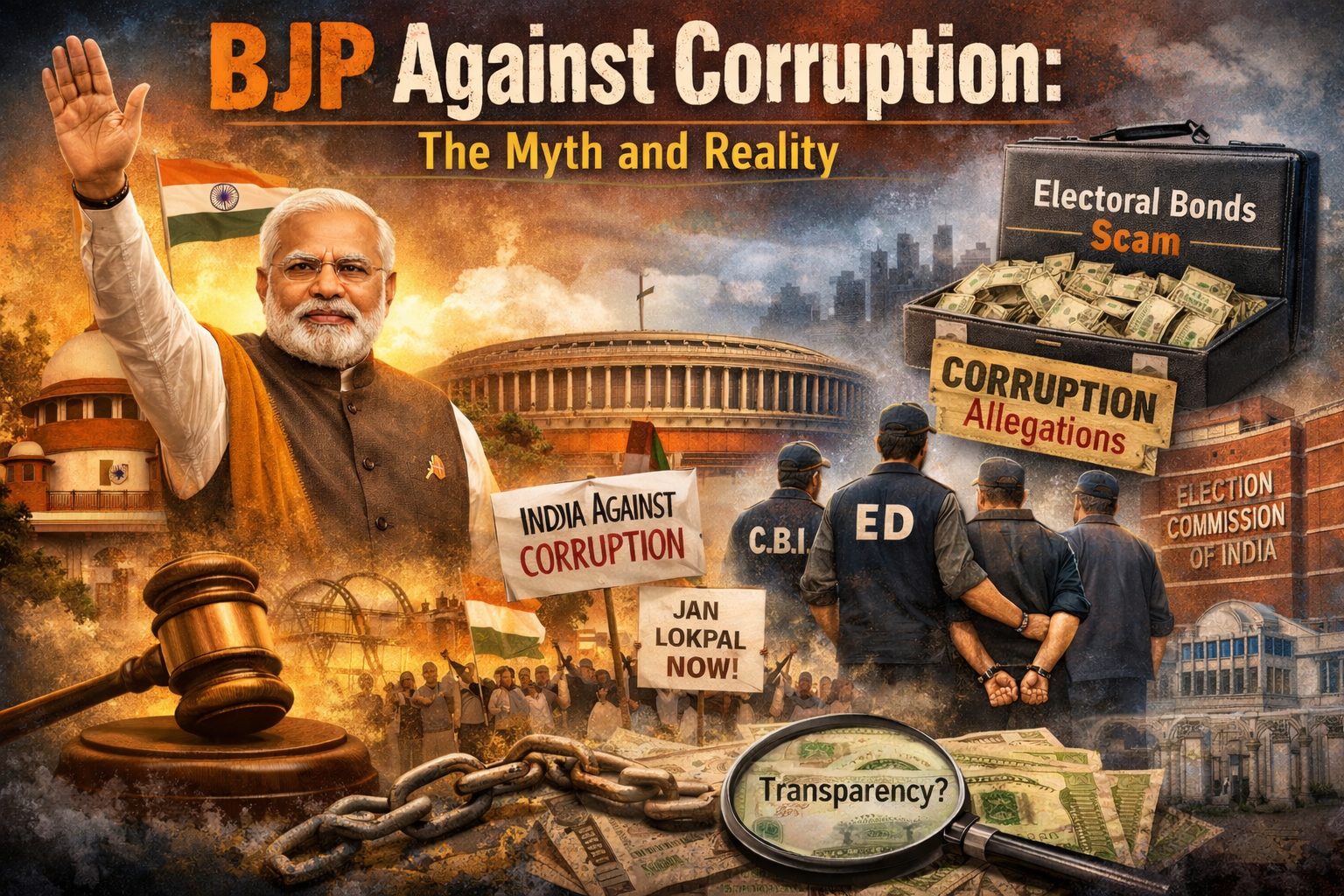
BJP Against Corruption: The Myth and Reality
9 Mar 2026





Media Wellness: Karmyoga In Action
24 Feb 2026


Niggles Heading Into Super Eights
23 Feb 2026

मुस्लिम परिवार ने हिंदू मंदिर के लिए दान की जमीन
20 Feb 2026

मोदी सरकार की हठधर्मिता ने संसद को कमजोर किया
20 Feb 2026
My Bookshelf
20 Feb 2026

Modi Govt. Intransigence undermines parliament
17 Feb 2026


ग्रीनलैंड से ट्रंप का क्या लेना-देना है?
14 Feb 2026



Communal Polarisation Has a Much-Feared Backlash
13 Feb 2026

West Asia: Pakistan Between Ambition and Reality
11 Feb 2026



The Right Course for Agitators in Iran
9 Feb 2026

पुस्तक समीक्षा
6 Feb 2026


Now Heading Towards T20 World Cup
4 Feb 2026




केसर बनाम केसर: शक्ति, धर्मपरायणता और अहंकार
31 Jan 2026


प्रत्यायन के पारिस्थितिकी तंत्र को समझना
31 Jan 2026
ईरान में आंदोलनकारियों के लिए सही रास्ता
31 Jan 2026

The Right Course for Agitators in Iran
29 Jan 2026
Understanding Ecosystem Of Accreditation
28 Jan 2026
Saffron Versus Saffron: Power, Piety, and Ego
28 Jan 2026






MY BOOKSHELF
16 Jan 2026




क्रिकेट के भीतर और आस पास का सर्कस
10 Jan 2026
न्यूयॉर्क की राजनीति, मुंबई में?
10 Jan 2026
वामपंथ की ताक़त की वापसी की तलाश
10 Jan 2026

Circus In And Around Cricket
7 Jan 2026

अरावली संकट: जब कानून प्रकृति के ख़िलाफ़
2 Jan 2026

वस्तुओं और सेवाओं के नियामकों की निष्पक्षता
2 Jan 2026
जब ज़हरीली हवा बने मुनाफ़े का साधन
2 Jan 2026


Impartiality Of Regulators In Goods And Services
31 Dec 2025



Cricket Selectors Continue to Baffle
24 Dec 2025

नए अमेरिका से भारत कैसे निपटे
19 Dec 2025
उत्तर प्रदेश की मतदाता सूची: योगी ने फोड़ा बम
19 Dec 2025

मेरी पत्रकारिता यात्रा
19 Dec 2025

झूठ के दौर में सच की लड़ाई
19 Dec 2025
My Bookshelf
19 Dec 2025

Electoral Rolls in U.P.: Yogi Drops a Bomb Shell
16 Dec 2025

How Should India Deal with Trump’s New America
16 Dec 2025


Vande Mataram: What's in a song?
15 Dec 2025
संजय गांधी – अनेक विरोधाभासों वाला व्यक्तित्व
12 Dec 2025


एक चुनाव जिसमें सब हार गए
12 Dec 2025
वंदे मातरम् : एक गीत में क्या रखा है?
12 Dec 2025

Dec 14: Sanjay Gandhi Birth Anniversary
11 Dec 2025


An Election That Everybody Lost
10 Dec 2025

अंतरराष्ट्रीय मानक : निष्पक्षता की धारणा
6 Dec 2025
डॉ. अम्बेडकर की पुण्यतिथि
6 Dec 2025
My Bookshelf
5 Dec 2025

December 6: Dr Ambedkar's death anniversary
3 Dec 2025
फील्ड मार्शल दिवाकर भट्ट नहीं रहे
29 Nov 2025

मुसलमानों में पिछड़ापन : एक समीपस्थ दृष्टि
29 Nov 2025

Backwardness Among Muslims: A Ring Side View
29 Nov 2025
आकाश के पार एक सलाम
28 Nov 2025
बिहार: चुनावी वादों की कठोर अर्थव्यवस्था
28 Nov 2025

Russia–Ukraine War: Hopes for Peace Strengthen
28 Nov 2025

A Salute Across Skies
25 Nov 2025

Bihar: The Harsh Economics of Electoral Promises
23 Nov 2025

India–Canada: Renewed Trust, Renewed Momentum
23 Nov 2025

एनडीए की अभूतपूर्व जीत कैसे संभव
23 Nov 2025
बिहार : वोट और सीटों का चौंकाने वाला असंतुलन
23 Nov 2025
MY BOOKSHELF
21 Nov 2025

Test Cricket: About Consistency and Hard Choices
18 Nov 2025
Bihar : Vote-seat Mismatch is Striking
16 Nov 2025
What Made Unprecedented Victory of NDA Possible
16 Nov 2025
आरएसएस प्रमुख का बड़ा इमेज-बिल्डिंग अभियान
14 Nov 2025
129वीं जयंती पर विशेष
14 Nov 2025
Nov 14 : Jawaharlal Nehru’s Birth Anniversary
13 Nov 2025

RSS Chief’s Big Image-Building Exercise
11 Nov 2025


खोजी पत्रकारिता का अवसान
10 Nov 2025
इस्लामोफ़ोबिया अब बढ़ती चिंता का कारण
7 Nov 2025
Sun Of Revolution Over Citadel Of Reaction
6 Nov 2025






दीवाली के दीयों संग जलती रिश्वत की लौ
1 Nov 2025
Islamophobia Now Being Seriously Challenged
1 Nov 2025

Zohran Mamdani’s Fight to Reclaim New York
29 Oct 2025
Bihar Politics: The Knock of Youth Leadership
29 Oct 2025





Understanding World Of Voluntary Standards
24 Oct 2025


भारत को स्थायी यूएनएससी सीट — लेकिन बड़ी कीमत पर
17 Oct 2025

बिहार की मतपरीक्षा: क्या बदल रहा है चुनाव आयोग?
17 Oct 2025





Godi Media’s Criminal Silence on Hate Crimes
15 Oct 2025
Making Indian Certifications Globally Acceptable
16 Oct 2025




ASIA CUP SELECTIONS IGNITE DEBATE
27 Aug 2025
GST-2: Revenue First or Relief for Consumers?
27 Aug 2025




Trump’s H-1B Visa Squeeze and Our Job Dilemma
20 Aug 2025


स्वतंत्रता: केवल राजनीतिक आज़ादी से परे
22 Aug 2025



Freedom: Beyond Political Independence
15 Aug 2025

Column: Front Foot Forward
13 Aug 2025


Monday Matters: India’s Junk Policy
14 Jul 2025

Monday Matters
4 Jul 2025


ThoughtfortheDay
27 Jun 2025
इज़राइल-ईरान युद्ध का असली विजेता कौन ?
27 Jun 2025
जीवन के सभी मुद्दों का स्थाई समाधान "भगवत गीता"
27 Jun 2025
ईरानी मिसाइलों ने दिया अडानी को जोर का झटका
27 Jun 2025
Who is the real victor of Israel-Iran War ?
27 Jun 2025

Besides Others, Iranian Missiles Hit Adani Hard
27 Jun 2025

Thought for the Day
25 Jun 2025



Thought for the Day
23 Jun 2025


अहमदाबाद एयर क्रैश और सूचना जगत की अराजकता
21 Jun 2025


Thought for the Day
20 Jun 2025


Thought for the Day
18 Jun 2025


Thought for the day
16 Jun 2025


गीता का ज्ञान अब आम आदमी के लिए सरल हुआ
14 Jun 2025

Thought for the Day
13 Jun 2025
Operation Sindoor Loses Much of Its Sheen
13 Jun 2025
Remembering the Emergency
13 Jun 2025

Thought for the Day
11 Jun 2025



Thought for the Day
9 Jun 2025




आईएसओ प्रमाणन : गरीब उपभोक्ताओं को धोखा देना
7 Jun 2025


Thought For the Day
6 Jun 2025

Thought for the Day
3 Jun 2025

Thought for the Day
2 Jun 2025



टेस्ट टीम चयन: कुछ सवाल अब भी अनुत्तरित
1 Jun 2025

आज नेहरू की इतनी आलोचना क्यों?
1 Jun 2025


Thought for the Day
31 May 2025

Is diluting POCSO for adolescents an option?
31 May 2025

Thought for the Day
28 May 2025


Thought for the Day
26 May 2025



अनीता आनंद कनाडा की पहली हिंदू विदेश मंत्री
26 May 2025

Thought for the Day
23 May 2025
War Ends, Election Campaign Begins
23 May 2025

Thought for the Day
21 May 2025


May 21: Rajiv Gandhi Martyrdom Day
21 May 2025

Choosing Test Captain A Problem For Selectors
20 May 2025

Thought for the Day
19 May 2025










Thought for the Day
16 May 2025


Uneasy Peace Prevails Between India and Pakistan
15 May 2025

Thought for the Day
14 May 2025

Pakistan Faces an Ideological Crisis of Identity
14 May 2025


Thought for the day
11 May 2025


Hidden Cost of the India-Pakistan Clash
11 May 2025
क्या राहुल गांधी मोदी का विकल्प हैं?
10 May 2025

भारतीयों ने कनाडा की संसद में 25 उम्मीदवार भेजे
10 May 2025

Thought for the day
7 May 2025
Is Rahul Gandhi an alternative to Modi?
7 May 2025

Thought for the Day
5 May 2025






साहित्य
3 May 2025

Thought for the day
3 May 2025

IMF Foresees Great World-Wide Depression
3 May 2025

Thought for the Day
1 May 2025


Thought for the Day
22 Apr 2025

Supreme Slipper Hurled at Hindutva Forces
22 Apr 2025

Thought for the Day
21 Apr 2025

April 19 : Charles Darwin Death Anniversary
21 Apr 2025


Thought for the Day
18 Apr 2025


Thought for the Day
16 Apr 2025


Thought for the Day
14 Apr 2025


Waqf Act: Two-way Pressure On JDU Muslim Leaders
14 Apr 2025
वक्फ बिल के खिलाफ तमिलनाडु का 'नरगिस खान अनुभव'
12 Apr 2025


Thought for the Day
11 Apr 2025
A common man’s prescription for inner peace
11 Apr 2025

Decisive Time for Left Forces in Indian Politics
11 Apr 2025

Thought for the Day
9 Apr 2025



वक्फ बिल द्वारा भाजपा के जनाधार को खतरा
9 Apr 2025

भारत के पूर्वी बेसिन में खनिज तेल की खोज।
9 Apr 2025

Thought for the day
9 Apr 2025

Waqf Bill May Wipe out BJP’s Mass Base
9 Apr 2025

Thought for the day
2 Apr 2025
Global Energy Scenario and Indian Economy
2 Apr 2025


Thought for the Day
31 Mar 2025



महा कुंभ और बीजेपी में उत्तराधिकार की जंग
29 Mar 2025




Thought for the Day
28 Mar 2025
Maha Kumbh and succession war in the BJP
28 Mar 2025


Thought for the Day
26 Mar 2025
Religious Fanaticism Harps on False Pride
26 Mar 2025

Thought for the day
24 Mar 2025

Trade with U.S: India Wants AI Gets Almonds
24 Mar 2025


Thought for the Day
21 Mar 2025
Should Not We Tell This Bully To Get Lost?
21 Mar 2025

Thought for the Day
19 Mar 2025
Modi And Trump's New World Order
19 Mar 2025

Exodus of Foreign Investors Continues
19 Mar 2025

Thought for the Day
17 Mar 2025


Political Turmoil Prevails In Maharashtra
17 Mar 2025
Usual Rahul Bashing By BJP To Defend Gujarat
12 Mar 2025

Thought for the Day
12 Mar 2025


Thought for the day
10 Mar 2025


International Women's Day
7 Mar 2025

Thought for the Day
7 Mar 2025

March 8: International Women’s Day
7 Mar 2025

Thought for the Day
5 Mar 2025
Trump-Zelenskyy public spat: What is ahead?
5 Mar 2025


Thought for the Day
3 Mar 2025


Thought for the Day
28 Feb 2025
Do They Really Deserve Our Sympathy ?
28 Feb 2025

New CEC’s Appointment Raising Ugly Questions
28 Feb 2025

Thought for the Day
26 Feb 2025
Women’s Rights Under Serious Threat
26 Feb 2025

Trump-Netanyahu Gaza Strategy Is A Failure
26 Feb 2025

Thought for the Day
25 Feb 2025



Thought for the Day
25 Feb 2025



Thought for the Day
19 Feb 2025

Congress rising from the ashes like Phoenix
19 Feb 2025

Thought for the Day
17 Feb 2025



Thought for the day
14 Feb 2025
Maha Kumbh And BJP’s Poll Prospects
14 Feb 2025

Delhi Polls: Heads I Win, Tails You Lose!
14 Feb 2025

Thought for the Day
12 Feb 2025
The Return of ‘Ugly American’
12 Feb 2025


Thought for the Day
10 Feb 2025

Deportation of Indians raises critical questions
10 Feb 2025
Bid To Undermine Mshatma Gandhi's Stature
10 Feb 2025

Thought for the Day
7 Feb 2025
Arvind Kejriwal an enigma of Indian politics
7 Feb 2025


Thought for the Day
5 Feb 2025


Thought for the Day
3 Feb 2025

The start of the tariff war
3 Feb 2025


Thought for the day
31 Jan 2025
BJP gives communal colour to Delhi elections
31 Jan 2025


Thought for the Day
29 Jan 2025


Thought for the Day
27 Jan 2025



Thought for the Day
24 Jan 2025

Delhi Elections: The Scene Is Very Much the Same
24 Jan 2025


Thought for the Day
22 Jan 2025

Devaluing political vocabulary- the RSS-BJP way
22 Jan 2025

30-Day Truce A New Dawn for Gaza
22 Jan 2025

Thought for the Day
20 Jan 2025

Political Rivalry Over Kumbh and Gangasagar Mela
20 Jan 2025

A Desperate Attempt to Please Trump
20 Jan 2025

Thought for the Day
17 Jan 2025


Uncouth By Choice Or compulsion ?
17 Jan 2025

Thought for the Day
14 Jan 2025
INDIA Bloc and its Contradictions
14 Jan 2025

Kasganj Case : Genises of an Unsavoury Incidence
14 Jan 2025

Thought for the day
12 Jan 2025
Winning An Election By Hook or Crook
12 Jan 2025


Thought for the Day
10 Jan 2025

भारत के सामने क्षेत्रीय भू-राजनीतिक चुनौतियां
10 Jan 2025

Chadar Politics and BJP Poll Prospects in Delhi
10 Jan 2025

Delhi elections crucial test for 3 stakeholders
10 Jan 2025

Thought for the Day
8 Jan 2025


कनाडा की नई अप्रवासन नीति का मतलब
8 Jan 2025

New Gig Economy is Slavery in New Garb
8 Jan 2025
Looking at Modi’s Many Contradictions
8 Jan 2025

Thought for the Day
6 Jan 2025


हास्य व्यंग
6 Jan 2025

Monday Musings
6 Jan 2025

Thought for the Day
3 Jan 2025
हैप्पी न्यू इयर!
3 Jan 2025

उम्मीद का साल 2025
3 Jan 2025

Using Social Media to Restore Media Health
3 Jan 2025

Thought for the day
2 Jan 2025



BJP’s negative politics and its impact on us
2 Jan 2025

Thought for the Day
30 Dec 2024

श्रद्धांजलि : डॉ मनमोहन सिंह
30 Dec 2024
दिसम्बर 30: जन्म दिवस
30 Dec 2024

Monday Musing
30 Dec 2024

Thought for the Day
27 Dec 2024


भारत-चीन संबंधों में सकारात्मक पहल
27 Dec 2024

Indian Economy in the shadow of crisis
27 Dec 2024

Thought for the Day
25 Dec 2024
भारतीय राजनीति के अजातशत्रु - अटल बिहारी वाजपेयी
25 Dec 2024

संविधान के 75 साल के बाद हम कहाँ हैं
25 Dec 2024

How Merry Is This Christmas
25 Dec 2024

Thought for the Day
23 Dec 2024
दिसम्बर 23 : चौधरी चरण सिंह जयंती
23 Dec 2024



SC Ruling Makes DND Flyway Toll-Free
23 Dec 2024

Thought for the day
20 Dec 2024


हास्य व्यंग
20 Dec 2024
Using Big Names for Sectarian Politics
20 Dec 2024


Thought for the Day
18 Dec 2024

दिसम्बर 15 : पुण्यतिथि
18 Dec 2024
Wednesday Wisdom
18 Dec 2024

After Rahul BJP’s Bugbear is Priyanka Gandhi
18 Dec 2024

Thought for the Day
16 Dec 2024

राष्ट्र की समृद्धि के लिए एक आध्यात्मिक उपाए
16 Dec 2024


Trump’s Tariff Threat Puts Canada In Active Mode
16 Dec 2024


Thought for the Day
13 Dec 2024



The Price of Privilege
13 Dec 2024


Thought for the day
11 Dec 2024
तोला मीशा माशा
11 Dec 2024

Why and how of Wednesday Wisdom
11 Dec 2024


Thought for the day
9 Dec 2024




Thought for the Day
5 Dec 2024


दिसंबर 6: डॉ. अंबेडकर पुण्यतिथि
5 Dec 2024
Friday Fuss
5 Dec 2024


Thought for the Day
4 Dec 2024




Thought for the day
2 Dec 2024

दिसंबर 3: मेजर ध्यानचंद पुण्यतिथि
2 Dec 2024
No cockroach Mukt Universe ever
2 Dec 2024
My friend Mr K Gopal Pandey
3 Dec 2024

Thought for the day
29 Nov 2024


Baloch Rebels May Sour China-Pakistan Bonhomie
29 Nov 2024
Need to be seen to be fair
29 Nov 2024

Thought for the Day
27 Nov 2024

तेज रफ्तार ले रही है हजारों लोगों की जान
27 Nov 2024



Thought for the Day
25 Nov 2024

विखंडित मणिपुर में शांति की तलाश
25 Nov 2024

हिंसा विरोधी महिला दिवस :25 नवम्बर
25 Nov 2024

Are We A Nation of Mediocre
25 Nov 2024

Thought for the Day
21 Nov 2024


Thought for the day
20 Nov 2024


ऊर्जा परिवर्तन: एक अच्छे भविष्य का मार्ग
20 Nov 2024


Thought for the day
19 Nov 2024

व्हाट्सएप का हमारे समाज पर नकारात्मक प्रभाव
19 Nov 2024

जुकाम का तरल उपचार
19 Nov 2024


November 19: Birthday
19 Nov 2024

Thought for the day
17 Nov 2024

19 नवम्बर: जन्मदिवस
17 Nov 2024

15 नवंबर, 1949
17 Nov 2024

November 14: Prayas Founders Day
17 Nov 2024


Thought for the Day
15 Nov 2024

नवम्बर 15 : गुरु नानक जयंती
15 Nov 2024


November 15: Guru Nanak's Birthday
15 Nov 2024
November 15: Guru Nanak Jayanti
15 Nov 2024

Thought for the day
14 Nov 2024

नवम्बर 14 : बाल दिवस
14 Nov 2024

नवम्बर 14 : बाल दिवस
14 Nov 2024

November 14: Nehru’s Birthday
14 Nov 2024

November 14: Nehru’s Birthday
14 Nov 2024

Thought for the Day
13 Nov 2024

झारखंड चुनाव 2024: चुनावी संघर्ष में कौन जीतेगा
13 Nov 2024


November 13: Maharaja Ranjit Singh’s Birthday
13 Nov 2024

Nehru’s birthday : November 14
13 Nov 2024

Thought for the Day
12 Nov 2024

अमेरिका में क्रिकेट
12 Nov 2024

Development Is Not By Financial Data Alone
12 Nov 2024


Thought for the Day
11 Nov 2024
नवम्बर 11 : शिक्षा दिवस
11 Nov 2024



Thought for the day
8 Nov 2024

नवम्बर 9:जयंती पर विशेष
8 Nov 2024



One Man's Vision Becomes Nation's Mission
8 Nov 2024

Thought for the Day
7 Nov 2024



Kashmiri Shaivism And Sufi Traditions
7 Nov 2024


Thought for the Day
5 Nov 2024
पुस्तक समीक्षा
6 Nov 2024




Thought for the Day
5 Nov 2024





Thought for the day
1 Nov 2024

पत्रकार आरिफ नकवी का बर्लिन में निधन !
1 Nov 2024




Thought for the day
30 Oct 2024

बलिदान दिवस : अक्टूबर 31
30 Oct 2024



Thought for the Day
29 Oct 2024

कौन तय करेगा अश्लीलता क्या है?
29 Oct 2024


Thought for the Day
25 Oct 2024

हास्य व्यंग
25 Oct 2024


Platform to combat sectarianism launched
25 Oct 2024


Thought for the Day
24 Oct 2024

बहराइच साम्प्रदायिक हिंसा
24 Oct 2024

अक्टूबर 19 : काफी हाउस का जन्मदिन
24 Oct 2024


Thought for the day
23 Oct 2024

क्या कश्मीरी पंडित घाटी में वापस जायँगे ?
23 Oct 2024

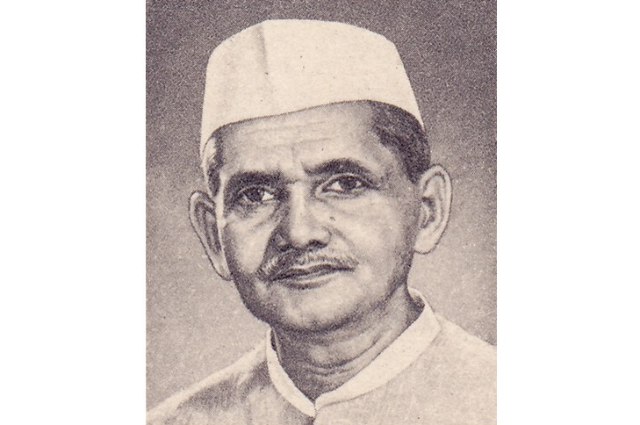
Shastri Ji is my father, my guru and my ideal
23 Oct 2024


Thought for the Day
22 Oct 2024

गाय भाजपा राजनीति का एक भावनात्मक मुद्दा
22 Oct 2024




Thought for the Day
21 Oct 2024





Thought for the Day
18 Oct 2024





Thought for the Day
17 Oct 2024
अक्टूबर 17 : महर्षि वाल्मीकि जयंती
17 Oct 2024
हास्य व्यंग
17 Oct 2024

How Deep Is The Hindu-Muslim Divide?
17 Oct 2024
Sir Syed Ahmad Khan : Oct 17 Birth Anniversary
17 Oct 2024

Thought for the Day
16 Oct 2024
शास्त्री जी मेरे पिता, मेरे गुरु और मेरे आदर्श
16 Oct 2024



No support To Waqf Bill, Says Hemant Soren
16 Oct 2024

Thought for the day
15 Oct 2024
नुक्कड़ नाटक
15 Oct 2024
हमारे देश में गांधी की छवि पर होते छद्म हमले !
15 Oct 2024



Thought for the day
14 Oct 2024





Thought for the day
11 Oct 2024

जन्मदिन अमिताभ बच्चन : अक्टूबर 11
11 Oct 2024

कनाडा में भारतीय भोजन की बहार
11 Oct 2024


Thought for the Day
10 Oct 2024
श्रद्धांजलि
10 Oct 2024

ईरान-इजराइल संघर्ष: अकेलेपन या घेराव का खेल?
10 Oct 2024


ICC women’s T20 world cup
10 Oct 2024

Thought for the Day
9 Oct 2024




Is the Indian Stock Market Crashing Again?
9 Oct 2024

Thought for the Day
8 Oct 2024

वायुसेना दिवस: अक्टूबर 8
8 Oct 2024

Who is A terrorist? Who is A traitor?
8 Oct 2024


Thought for the Day
7 Oct 2024


How I Rediscovered Mahatma Gandhi
7 Oct 2024

Thought for the Day
4 Oct 2024
प्रेरक प्रसंग.....
4 Oct 2024


Thought for the Day
3 Oct 2024




Thought for the Day
2 Oct 2024

अयोध्या गैंगरेप मामले से भाजपा मुश्किल में
2 Oct 2024

Thought for the Day
1 Oct 2024


इश्क कीजे फिर समझिए, जिंदगी क्या चीज है...
1 Oct 2024


Thought for the Day
27 Sep 2024


Thought for the Day
26 Sep 2024

सितम्बर 26 : डॉ. मनमोहन सिंह जन्मदिन
26 Sep 2024



House of Commons up against PM Justin Trudeau
26 Sep 2024
Thought for the Day
25 Sep 2024

देव आनंद जयंती : सितम्बर 26
25 Sep 2024

Godi media’s campaign of lies On Waqf Lands
25 Sep 2024
Thought for the Day
24 Sep 2024

व्यंग्य, विसंगतियों का बैरोमीटर
24 Sep 2024
Amit Shah Loses Face as Selja rejects BJP offer
24 Sep 2024

Adulterated Ghee Racket is worth Rs 5 Lakh Crore
24 Sep 2024
Thought for the Day
20 Sep 2024

हास्य व्यंग
20 Sep 2024

“Nearly 6 crore emails On Waqf Amendment Bill”
20 Sep 2024

Thought for the Day
19 Sep 2024

हरियाणा चुनाव में भाजपा की स्थिति नाज़ुक
19 Sep 2024



Thought for the Day
18 Sep 2024


दिल्ली में केजरिवल का ऐलान-ए-जंग
18 Sep 2024


Thought for the Day
16 Sep 2024

स्वतंत्र हिंदू द्वीप था अंडमान !
16 Sep 2024


Thought for the day
13 Sep 2024



A True Mass leader Sitram Yechury is no more
13 Sep 2024

Thought for the day
12 Sep 2024

पुस्तक पर चर्चा
12 Sep 2024

वर्षा ऋतु में स्वस्थ रहने के सरल उपाय
12 Sep 2024

Rahul Attacks China Policy Of Modi Govt.
12 Sep 2024

When Overseas Indians Do Their Bit
12 Sep 2024

Thought for the day
11 Sep 2024


क्या विध्वंस की आड़ में हो रहा है न्याय का हनन?
11 Sep 2024



Thought for the Day
10 Sep 2024

जाति आधारित जनगणना और आरएसएस की उलटबाँसियाँ
10 Sep 2024

Media under Modi: What lies ahead?
10 Sep 2024


Thought for the Day
6 Sep 2024




Thought for the Day
5 Sep 2024
शिक्षा दिवस : सितम्बर 5
5 Sep 2024

Teachers Day : Sept 5
5 Sep 2024

Why Our Politicians Are Corrupt And Crafty
5 Sep 2024

Thought for the Day
4 Sep 2024

क्षणिका
4 Sep 2024

सितम्बर पखवाड़ा
4 Sep 2024

कंगना बनी बीजेपी के लिए समस्या
4 Sep 2024


How to restore Credibility of TV News Media
4 Sep 2024

Thought for the Day
3 Sep 2024




Politics: Of Being Envious And Not To Be
3 Sep 2024

Thought for the Day
2 Sep 2024


हास्य व्यंग
2 Sep 2024

Let Us Learn To Respect Regional Sentiment
2 Sep 2024


Thought for the Day
30 Aug 2024
पुस्तक समीक्षा
30 Aug 2024
क्या सुंदरता के पैमाने पर इतिहास कुछ कहता है?
30 Aug 2024



Thought for the day
29 Aug 2024

अगस्त 29 : ध्यानचंद जयंती
29 Aug 2024
कुरुक्षेत्र का लाक्षाग्रह!
29 Aug 2024

Death is not just a number say women in Ukraine
29 Aug 2024

Thought for the Day
28 Aug 2024

अगस्त 26: मदर टेरेसा जयंती
28 Aug 2024




Thought for the Day
27 Aug 2024

यात्रा- वृतांत श्रावस्ती : बुद्ध का प्रिय स्थल
27 Aug 2024

गठबंधन की शल्य क्रिया
27 Aug 2024


Is BJP caught in the web of its own making?
27 Aug 2024

Thought for the day
22 Aug 2024


दुनियाभर में बिखरी भारतीय आमों की मिठास
22 Aug 2024



Thought for the Day
21 Aug 2024
अगस्त 19: खय्याम पुन्यतिथि
21 Aug 2024


80th Birthday Tribute
21 Aug 2024

Thought for the Day
20 Aug 2024
अगस्त 20 : जन्म दिवस पर विशेष
20 Aug 2024
हरिशंकर परसाई जन्म शताब्दी
20 Aug 2024


Reclaiming What Already Belongs To Women
20 Aug 2024

Thought for the Day
19 Aug 2024


प्रख्यात कवि रामदरश मिश्र शतायु हुए
19 Aug 2024

Women Suffering in Modi Rule, says AIDWA Report
19 Aug 2024


Thought for the day
16 Aug 2024

पेरिस ओलंपिक्स में भारत का निराशाजनक प्रदर्शन
16 Aug 2024

Role of Muslims in freedom movement highlighted
16 Aug 2024

Media Map Notice
14 Aug 2024

Thought for the day
14 Aug 2024


स्वतंत्र दिवस पर विशेष
14 Aug 2024

2024 Olympic Games
14 Aug 2024

U.S. Behind Her Ouster, Says Hasina
14 Aug 2024

Thought for the day
13 Aug 2024


तेहरान में हमास नेता की हत्या से बढ़ी अस्थिरता
13 Aug 2024


2024 Olympic Games
13 Aug 2024

Thought for the day
12 Aug 2024

अगस्त 11 : खुदीराम बोस बलिदान दिवस
12 Aug 2024

1 अगस्त : कमला नेहरू जन्मगांठ
12 Aug 2024



Thought for the Day
9 Aug 2024



Et Tu Putin
9 Aug 2024


Thought for the Day
8 Aug 2024



Thought for the Day
7 Aug 2024


Cat women and having children
7 Aug 2024

2024 Olympic Games
7 Aug 2024

Lessons We Need To Learn from Bangladesh
7 Aug 2024

Thought for the day
6 Aug 2024

2024 ओलंपिक खेल
6 Aug 2024

आखिर हसीना को जाना ही पड़ा
6 Aug 2024

लघु प्रसंग
6 Aug 2024



Thought for the day
5 Aug 2024
अगस्त 4: किशोर कुमार जन्मदिवस
5 Aug 2024


हास्य व्यंग
5 Aug 2024

24 Olympic Games
5 Aug 2024


Thought for the Day
2 Aug 2024



2024 Olympic Games
2 Aug 2024


Thought for the Day
1 Aug 2024
जुलाई 31: मोहम्मद रफ़ी पुण्यतिथि
31 Jul 2024


2024 Olympic Games
31 Jul 2024


Thought for the Day
31 Jul 2024
जुलाई 31: शहीद उधम सिंह बलिदान दिवस
31 Jul 2024

विविधता के लिए बहुसंख्यकवाद एक खतरा
31 Jul 2024

2024 Olympic Games
31 Jul 2024


Thought for the Day
29 Jul 2024

कमज़ोर सरकार का मजबूर बजट
29 Jul 2024

आखिर राज्यपाल बनवारीलाल पुरोहित की हो गयी छुट्टी
29 Jul 2024

Olympic Games-2024
29 Jul 2024

Thought for the Day
26 Jul 2024
जुलाई 27: अमजद खान की पुण्यतिथि
26 Jul 2024
“सियासत में कुर्सी बदलने में देर नहीं लगती”
26 Jul 2024



Thought for the Day
24 Jul 2024

योगी सरकार पर सुप्रीमकोर्ट का बुलडोज़र
24 Jul 2024


Olympic Games-2024
24 Jul 2024


Thought for the day
24 Jul 2024

गंगाजल की विशेषता और कावड़ यात्रा
24 Jul 2024

योगी ने अपनी साख बचाने के लिए मोदी को फंसा दिया
24 Jul 2024


Modi’s Moscow Visit Irks U.S. Armament Lobby
24 Jul 2024
Thought for the day
22 Jul 2024
जुलाई 23: महमूद की पुण्यतिथि
22 Jul 2024

नेपाल ने उत्तरी सीमा पर भारत का सिरदर्द बढ़ाया
22 Jul 2024
July 23: Gen. Dyer's Death Anniversary
22 Jul 2024


Thought for the Day
22 Jul 2024

भाजपा राजनीति का नया मोहरा - कांवड़ यात्रा
22 Jul 2024

पुरोला “लव जिहाद” मामला अदालत में गलत साबित
22 Jul 2024



Thought for the day
19 Jul 2024

जुलाई 21: गुरु पूर्णिमा पर विशेष
19 Jul 2024

अवध के नवाबों का मोहर्रम में योगदान
19 Jul 2024

कविता
19 Jul 2024
National Initiative for Communal Harmony Lunched
19 Jul 2024


Thought for the day
18 Jul 2024

मुहर्रम पर ताज़िया क्यों निकाला जाता है ।
18 Jul 2024
राजनीतिक भ्रष्टाचार एक बड़ी चुनौती
18 Jul 2024
लघु प्रसंग
18 Jul 2024

July 18: Rajesh Khanna's death anniversary
18 Jul 2024

Thought for the day
16 Jul 2024


अमेरिका को रास नहीं आई भारत और रूस की दोस्ती
16 Jul 2024
लघु प्रसंग
16 Jul 2024



Thought for the day
15 Jul 2024
राजनीति की कहानी फिल्मों की जुबानी
15 Jul 2024


लघु प्रसंग
15 Jul 2024



Thought for the Day
12 Jul 2024

जुलाई 12: दारा सिंह की पुण्यतिथि पर विशेष
12 Jul 2024

लघु प्रसंग
12 Jul 2024

क्षणिका
12 Jul 2024


Thought for the Day
11 Jul 2024

कश्मीर : मोदी के दावे के बावजूद बढ़ता आतंकवाद
11 Jul 2024

SEBI's responsibility increases as Sensex surges
11 Jul 2024

Muted Welcome To Labour Victory In India
11 Jul 2024

Thought for the Day
10 Jul 2024

रेल की रेलमपेल के बाद भी रेल ,रेल है !
10 Jul 2024



Thought for the Day
8 Jul 2024

वाजिद अली शाह और गलौती कबाब
8 Jul 2024

JULY 9: DEATH ANNIVERSARY
8 Jul 2024


Thought for the Day
8 Jul 2024

सेक्युलर राजनीति के लिए शुभ संकेत
8 Jul 2024

जुलाई माह: रथयात्रा के अवसर पर
8 Jul 2024

July 6: Dalai Lama's Birthday
8 Jul 2024

Thought for the Day
5 Jul 2024

अंधविश्वास के प्रबल विरोधी स्वामी विवेकानन्द
5 Jul 2024

July 4: Death Anniversary
5 Jul 2024

Will the U.S. get its first Woman President?
5 Jul 2024

Thought for the Day
4 Jul 2024
जुलाई 4: पूर्णतीथी
4 Jul 2024


क्षणिका
4 Jul 2024



Thought for the Day
3 Jul 2024

हम सभ्हल के चले सजन बरसात में!
3 Jul 2024


Rathyatra Festival
3 Jul 2024

How to restore Credibility of TV News Media.
3 Jul 2024

Thought for the Day
2 Jul 2024
मोदी 3.0 : ‘तीन तिगाड़ा काम बिगाड़ा
2 Jul 2024

30 जून: नागार्जुन के जन्म दिन की स्मृति में-
2 Jul 2024

Sant Nam Dev Purnya Thiti: July 3
2 Jul 2024


वर्ल्ड कप 2024:
1 Jul 2024

व्यंग्य
1 Jul 2024

कविता
1 Jul 2024
T20 World Cup:
1 Jul 2024

Rahul Gandhi: A leader whose time has come
1 Jul 2024

Thought for the Day
28 Jun 2024



T20 World Cup:
28 Jun 2024


Thought for the Day
27 Jun 2024

सरकार और प्रतिपक्ष समावेश से टकराव की ओर
27 Jun 2024

आपातकाल (1975-77) की मेरी यादें
27 Jun 2024

June 27 :Maharaja Ranjit Singh Death Anniversary
27 Jun 2024

Political challenges mount for Modi
27 Jun 2024

Thought for the Day
26 Jun 2024
आटा चक्की से डिजिटल साहित्यिक चक्की तक का सफर
26 Jun 2024
Book Review
26 Jun 2024


Thought for the Day
25 Jun 2024
23 जून: संजय गाँधी पुण्यतिथि
25 Jun 2024
हास्य व्यंग
25 Jun 2024

क्षणिका
25 Jun 2024



Thought for the Day
24 Jun 2024

२२ जून: संत कबीरदास जी जयंती
24 Jun 2024

पाकिस्तान का भविष्य: वैचारिक शून्यता और भटकाव
24 Jun 2024


One Nation, One Test Too Tough To Hold In India
24 Jun 2024

Thought for the Day
21 Jun 2024

21 जून: अंतर्राष्ट्रीय योग दिवस
21 Jun 2024




Thought for the Day
20 Jun 2024

अंधेरे में तीर चलाने का प्रयास करते ज्योतिषी
20 Jun 2024



Special on World Sauntering Day (June 19)
20 Jun 2024

Thought for the Day
19 Jun 2024
पाकिस्तान के सामने वैचारिक अस्तित्व का संकट
19 Jun 2024
परसाई मार्ग वहां जहां उनके घर का नामो निशान नहीं
19 Jun 2024

T20 World Cup
19 Jun 2024


Thought for the Day
18 Jun 2024
साहित्यिक लाग डाट
18 Jun 2024


कविता
18 Jun 2024

New Petroleum Pricing Regime Likely
18 Jun 2024

Maharashtra: Why Rebel Leaders Will Not Succeed
18 Jun 2024

Thought for the Day
17 Jun 2024
जून 14 : जन्मदिवस
17 Jun 2024

लोकसभा चुनाव: महागठबन्धन की राजनीति में बैसाखी
17 Jun 2024

क्षणिका
17 Jun 2024
June 16: World Father’s Day
17 Jun 2024
An Exclusive Interview
17 Jun 2024

Thought for the Day
14 Jun 2024

जून 14 :विश्व रक्तदान दिवस
14 Jun 2024

Mr Mohan Bhagwat, you Have spoken too late !
14 Jun 2024


Thought for the Day
13 Jun 2024
श्रीमान भागवत जी , आप बहुत देर से बोले
13 Jun 2024


क्षणिकाऐ
13 Jun 2024

RSS and Modi’s BJP Tussle out in the open
13 Jun 2024

Thought for the Day
12 Jun 2024

मायावती के कारण इंडिया अलायन्स को हुआ भरी नुकसान
12 Jun 2024

नई लोक सभा में मोदी की मनमानी चलना मुश्किल
12 Jun 2024

Children’s world
12 Jun 2024


Thought for the Day
11 Jun 2024

दूरदर्शन और सिनेमा एक प्रदूषण का स्त्रोत
11 Jun 2024


OPP. WANTS STOCK PROBE
11 Jun 2024

Mayawati Alienates Muslim leaders
11 Jun 2024

Thought for the Day
10 Jun 2024





Thought for the Day
7 Jun 2024

हास्य व्यंग
7 Jun 2024

मोदी के राजनीतिक कौशल की कड़ी परीक्षा का समय
7 Jun 2024

“Modi’s Political Career All But Over”
7 Jun 2024




क्षणिकाऐ
6 Jun 2024

Modi’s political skills under severe test?
6 Jun 2024


Thought for the Day
4 Jun 2024

जॉर्ज, मोदी, राजग की जीत और मैं !
4 Jun 2024

क्षणिकाऐ
4 Jun 2024


Thought for the Day
3 Jun 2024
जन्म : 3 जून 1930 स्वर्गवास 29 जनवरी 2019
3 Jun 2024

चुनाव 2024 : एग्जिट पोल कुछ सवाल
3 Jun 2024

क्षणिकाऐ
3 Jun 2024


Thought for the Day
31 May 2024

रवीन्द्र नाथ त्यागी की चुहलबाजी !
31 May 2024

श्रणिका
31 May 2024

60th Death Anniversary Tribute
31 May 2024


डबल इंजन सरकार मे महिलाओं पर अत्याचार
30 May 2024
मई 29: एक ऐतिहासिक और विलक्षण दिवस
30 May 2024

क्षणिका
30 May 2024
Porsche car case: How media should not report.
30 May 2024


Thought for the Day
29 May 2024

क्षणिकाऐ
29 May 2024

हास्य व्यंग्य
29 May 2024


Thought for the Day
28 May 2024

मतदान पहले और अब मोदी राज में
28 May 2024
27 मई : 60वीं पुण्यतिथि
28 May 2024

Baby Reindeer :Male Stalking Makes World News
28 May 2024

Thought for the day
27 May 2024

चुनाव: ऊंट जाने किस करवट बैठेगा ?
27 May 2024

“चाय ही चाय हाय हाय।
28 May 2024

क्षणिका
27 May 2024


Thought for the day
24 May 2024





Thought for the day
23 May 2024

बुद्ध पूर्णिमा: शांति और प्रेरणा का पर्व
23 May 2024
चुनाव: तमिलनाडु की राह पर चलता हुआ आंध्र प्रदेश
23 May 2024

क्षणिका
23 May 2024


Will the Real Prashant Kishor Please Stand Up?
23 May 2024
Thought for the day
22 May 2024


Covishield: ICMR role under scanner
22 May 2024

क्षणिका
22 May 2024

दूध की नहरें या चूने का पानी
22 May 2024

हास्य व्यंग्य
22 May 2024
Thought for the day
21 May 2024


Many A Twist In Swati Maliwal’s Tale
21 May 2024

क्षणिका
21 May 2024

हास्य व्यंग
21 May 2024

मस्तिष्क एक हिंदी पत्रिका के संपादक का
21 May 2024
Thought for the day
20 May 2024
रचना कर्म की नियति
20 May 2024

तूफ़ान अल-अक़सा : ऐतिहासिक संदर्भ सामयिकी
20 May 2024


Why and how Andhra is going the TN way
21 May 2024
Thought for the Day
17 May 2024

चल बसी नोबेल पुरस्कार विजेता एलिस मुनरो
17 May 2024


क्षणिका
17 May 2024

Grim Realities Belie Claims of Economic Progress
17 May 2024

Elections 2024
17 May 2024
Thought for the day
16 May 2024

India Fails to Tackle Problem of Brain Drain
16 May 2024

क्षणिकाऐ
16 May 2024


मणिशंकर वीडियो : भाजपा का बिना बात का मुद्दा
16 May 2024
Thought for the day
15 May 2024

संस्मरणो का अनूठा जाल !
15 May 2024

क्षणिकाऐ
15 May 2024


दिन का विचार
13 May 2024
सूरज की परछाई ही वक्त नापेंगी
13 May 2024

जन सराकारों से ध्यान हटाने की कोशिश
13 May 2024

क्षणिकाएं
13 May 2024

Mothers Day : May 12
13 May 2024




क्षणिकाएं
10 May 2024


Thought for the Day
9 May 2024

हास्य व्यंग
9 May 2024
नज़्म
9 May 2024


Thought for the Day
8 May 2024

लघु प्रसंग
8 May 2024

बेरहम राजनीति और घोषणापत्रों की तबालत
8 May 2024



Thought for the Day
7 May 2024
कुर्सी का यह नया कुरुक्षेत्र
7 May 2024
लघु प्रसंग
7 May 2024
दौर-ए-इलेक्शन
7 May 2024

Thought for the Day
6 May 2024
नेपाली करेंसी नोटों पर 'नया मानचित्र'
6 May 2024


क्षणिकाएं
6 May 2024
Campaign to Defend Constitution Launched
6 May 2024
Jobs Abroad for Indians To Become Scarce
6 May 2024
Thought for the Day
2 May 2024

दिल्ली के स्कूलों को बम से उड़ाने की धमकी
2 May 2024

घृणास्पद भाषणों का लोकतंत्र पर प्रभाव
2 May 2024

क्षणिकाएं
2 May 2024

Why do ex-servicemen shy away from politics?
2 May 2024

Dirty Tricks Department on an overdrive?
2 May 2024
Thought for the Day
1 May 2024

1 मई : मजदूर दिवस
1 May 2024

Why Modi Is targeting Sharad Pawar ?
1 May 2024

Hate Speech and Its Impact on Democracy
1 May 2024
Thought for the Day
30 Apr 2024

लोकसभा 2024: चुनाव का बदलता हुआ चेहरा
30 Apr 2024


क्षणिकाएं
30 Apr 2024

FIRs Must be Taken with a Pinch of Salt
30 Apr 2024

Rare Display of Statesmanship by Kharge
30 Apr 2024
Thought for the Day
29 Apr 2024
ईसी’ पेपर: इतनी जल्दी क्या थी चुनाव आयोग को
29 Apr 2024
सिख और उनका सैन्य इतिहास
29 Apr 2024

क्षणिकाएं
29 Apr 2024


Can there be a Working Consensus on Plastics?
29 Apr 2024
Thought for the Day
25 Apr 2024

माल कल्चर:लैया रामदाने की !
25 Apr 2024
ओलम्पिक खेल :पेरिस 1924 - पेरिस 2024
25 Apr 2024


Invisible Christians in Lok Sabha Elections
25 Apr 2024
Thought for the Day
24 Apr 2024
पहले चरण के बाद मोदी की घबराहट
24 Apr 2024
अंग्रेज गये तो अंग्रेजी भी चली जानी चाहिये।
24 Apr 2024

श्रणिका
24 Apr 2024

“Look For Reasons To Smile And Find A Thousand.”
24 Apr 2024
How Formidable BJP Looks In Ongoing Elections
24 Apr 2024
Thought for the Day
23 Apr 2024

शहाना बीमारी है दर्दे दिल !
23 Apr 2024
जूलियस रेबेरो ने प्रधान मंत्री से क्या कहा?
23 Apr 2024

श्रणिका
23 Apr 2024

Influencer Marketing
23 Apr 2024
Thought for the Day
22 Apr 2024

इंडिया पुनः भारत कब बनेगा
22 Apr 2024

गोद में उसकी…..
22 Apr 2024

लघु प्रसंग
22 Apr 2024


Thought for the Day
19 Apr 2024

कौशल शिक्षा का पूरक है
19 Apr 2024

श्रणिका
19 Apr 2024

LET US LEARN TO RESPECT REGIONAL SENTIMENTS
19 Apr 2024
Olympic Games :Paris 1924 vs. Paris 2024
19 Apr 2024
Thought for the Day
18 Apr 2024


राजभाषा की छौंक बघार !
18 Apr 2024


Thought for the Day
17 Apr 2024
"बिलखतीं टूटी ईंटों के वेदनामय स्वर"
17 Apr 2024

भारत के भविष्य को आकार देता हमारा मतदाता
17 Apr 2024

श्रणिका
17 Apr 2024

Thought for the Day
16 Apr 2024

समस्याओं की बेड़ियों में जकड़ी है भारत की प्रगति
16 Apr 2024

सीएसडीएस की चुनाव समीक्षा से उठते सवाल
16 Apr 2024

श्रणिका
16 Apr 2024
Do Our Elections Shun Reality and Promise Moon ?
16 Apr 2024

Shaping India's Future Through Voting
17 Apr 2024
Thought for the Day
15 Apr 2024
“मुस्कुराने के कारण ढूंढिए आपको हजार मिलेंगे "
15 Apr 2024

धीरे-धीरे एक वैश्विक उत्सव बनता वैसाखी त्योहार
15 Apr 2024

श्रणिका
15 Apr 2024


Thought for the Day
12 Apr 2024
अब बुरे फंसे बाबा राम देव जी
12 Apr 2024
चरण स्पर्श और आशीर्वाद से सुधरती सेहत
12 Apr 2024

श्रणिका
12 Apr 2024


Thought for the Day
11 Apr 2024
राजनीती की परम्पराओं पर लगा ग्रहण !
11 Apr 2024

पंजाब की राजनितिक के ठेकेदार
11 Apr 2024

श्रणिका
11 Apr 2024

War In Gaza: Jordan in a Catch 22 Situation
11 Apr 2024
Thought for the Day
10 Apr 2024

अखिलेश यादव : संभावनाएं और चुनौती
10 Apr 2024

श्रणिका
10 Apr 2024
Massive unemployment in India worries World Bank
10 Apr 2024

Thought for the Day
9 Apr 2024

भाषा का कटोरा
9 Apr 2024

श्रणिका
9 Apr 2024

How Top Leaders Are Shaming India
10 Apr 2024
Thought for the Day
8 Apr 2024
हास्य व्यंग
8 Apr 2024

Elections 2024: Kharge May Be The Next PM
8 Apr 2024
Thought for the Day
5 Apr 2024


श्रणिकाऐ
5 Apr 2024

Thought for the Day
4 Apr 2024

चुनाव मैदान में यह विचित्र उम्मीदवार
4 Apr 2024

स्वस्थ जगत
4 Apr 2024

श्रणिकाऐ
4 Apr 2024

Thought for the Day
3 Apr 2024

हास्य व्यंग
3 Apr 2024


लघु प्रसंग
3 Apr 2024
More a research treatise than a book
3 Apr 2024

Thought for the Day
2 Apr 2024

अत्यधिक गर्म महीनों में पर्यटन सीजन
2 Apr 2024

मूर्खता का त्योहार अप्रैल फूल
2 Apr 2024

श्रणिका
2 Apr 2024


Market Boom Fails To Create Jobs In India
2 Apr 2024
Thought for the Day
1 Apr 2024

वर्ष 2024 के चुनाव की अभूतपूर्व पृष्ठभूमि
1 Apr 2024

BJP’s 400-Seat Claim Unrealistic And fake
1 Apr 2024
Thought for the Day
29 Mar 2024



श्रणिका
29 Mar 2024

सिंदूर पर फिजूल का कानूनी विवाद !
29 Mar 2024

Thought for the Day
28 Mar 2024

चुनावी बॉन्ड : बाजार बनती हमारी राजनीति
28 Mar 2024


श्रणिका
28 Mar 2024


Poll-eve Defections An Unresolved Problem
28 Mar 2024
Thought for the Day
27 Mar 2024
विकास के दावे और नागरिकता छोड़ते हमारे नागरिक
27 Mar 2024

अनेक अड्डे हैं लखनऊ में बैठकबाजी के
27 Mar 2024

श्रणिका
27 Mar 2024
Understanding JNU Student Union Election Results
27 Mar 2024

Thought for the Day
26 Mar 2024

न्यायपालिका और प्रशासन के बीच चलती तीखी जंग
26 Mar 2024

बुरा ना मानो होली है।
26 Mar 2024

Is Corporate Money Dictating Governance?
26 Mar 2024

Pak -Afghan Tension Escalates With Air Strikes
26 Mar 2024
Thought for the Day
22 Mar 2024

केजरीवाल की गिरफ़्तारी से उठते प्रश्न
22 Mar 2024

यह वर्ष 2024 की होली या चुनावी होली
22 Mar 2024

फागुन में मस्ती चढ़ी!
22 Mar 2024

Thought for the Day
21 Mar 2024
मानो तो मौज़ है, वरना समस्या तो हर रोज है।
21 Mar 2024

हास्य व्यंग
21 Mar 2024

श्रणिका
21 Mar 2024
Lok Sabha Battle In U.P. - A Reality Check
21 Mar 2024
Thought for the Day
20 Mar 2024
पुण्यतिथि :17 मार्च हिमालय का चन्दन हेमवती नन्दन
21 Mar 2024

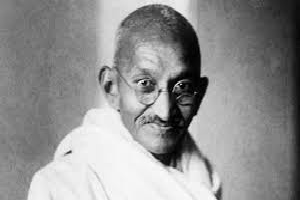
महात्मा गांधी की भूमि में एक अक्षम्य अपराध
20 Mar 2024

व्यंग
20 Mar 2024

Gaza War : Sweet Dates Turn Bitter For Israel
20 Mar 2024
V.P. Prabhakar -a “gentleman journalist “
20 Mar 2024
Thought for the Day
19 Mar 2024

An Unpardonable Act in Land of Mahatma Gandhi
19 Mar 2024

Punjab : Battle Lines Yet To Be Drawn
19 Mar 2024

श्रणिकाऐ
19 Mar 2024

हास्य व्यंग
19 Mar 2024
Thought for the Day
18 Mar 2024

आवश्यकता है पाकिस्तान से सम्बन्ध सुधारने की
18 Mar 2024

आत्म मुग्धता
18 Mar 2024


Thought for the Day
15 Mar 2024
नागरिकता संशोधन अधिनियम क्यों असंवैधानिक है
15 Mar 2024

श्रणिका
15 Mar 2024

Manner of Appointment of ECs Comes Under Fire
15 Mar 2024

Thought for the Day
13 Mar 2024

दाण्डी मार्च की सालगिरह
13 Mar 2024
संस्कृति का उपनिवेशीकरण या अधिनायकवाद की ओर
13 Mar 2024

श्रणिका
13 Mar 2024
Democracy : A World In Transition Period
13 Mar 2024
Regime Change in Haryana: Split Or “Fixed Fight”
13 Mar 2024
Thought for the Day
12 Mar 2024
एक सम्मोहक व्यक्तित्व के धनि अज्ञेय
12 Mar 2024

आम जन के अधिकारों के प्रहरी भारतीय न्यायालय
12 Mar 2024

श्रणिका
12 Mar 2024

BJP Biggest Gainer of Funds From Unknown Sources
12 Mar 2024
Thought for the Day
11 Mar 2024


63वीं पुण्यतिथि पर विशेष.......
11 Mar 2024

श्रणिकाऐ
11 Mar 2024


Thought for the Day
8 Mar 2024

समस्या है हमारी नई शहरी मलिन बस्तियाँ
8 Mar 2024

अमेरिका में असुरक्षित होता हमारा जीवन
8 Mar 2024

श्रणिकाऐ
8 Mar 2024

Will We Ever Get Rid Of Corruption?
8 Mar 2024

Thought for the Day
7 Mar 2024


जो रचेगा, सो बचेगा
7 Mar 2024

श्रणिका
7 Mar 2024


Thought for the Day
6 Mar 2024

भारतीय मुसलमान और चुनावी विकल्प
6 Mar 2024
एक उपेक्षित उपन्यासकार की बरसी !
6 Mar 2024

Overseas Punjabis reviving sports in Punjab
6 Mar 2024
Is Deification in the Indian DNA?
6 Mar 2024
Thought for the Day
5 Mar 2024

हास्य व्यंग्य
5 Mar 2024

मेरे पिया गए रंगून वह से आया टेलीफोन…..
5 Mar 2024

Insecure Indian Lives Getting in the U.S.
5 Mar 2024
Thought for the Day
4 Mar 2024

हास्य व्यंग्य
4 Mar 2024

चुनाव 2024 : युवा वोटर तय करेगा देश की दिशा
4 Mar 2024
श्रणिकाऐ
4 Mar 2024

Thought for the Day
2 Mar 2024
“एमएईएफ को बंद करने का निर्णय छात्र विरोधी "
2 Mar 2024

रास्ता ही मेरा घर है!
2 Mar 2024

Robust Growth Rate Marred By High Inflation
2 Mar 2024

NGOs Help Bring J & K Youth to Mainstream
2 Mar 2024
Thought for the Day
29 Feb 2024

राहुल गांधी की यात्रा में अर्चन डालती भाजपा
29 Feb 2024
संकट का “अच्छा उपयोग” करते एकाधिकारी घराने
29 Feb 2024

बैठे-ठाले
29 Feb 2024

Election Year: Tractors choke EU roads too
29 Feb 2024

Thought for the Day
28 Feb 2024
पंजाब की राजनीति से फ़िल्मी सितारों की बिदाई
28 Feb 2024


श्रणिका
28 Feb 2024


Thought for the Day
27 Feb 2024
हम ध्वनि प्रदूषण की अनदेखी क्यों करते हैं?
27 Feb 2024
दुनिया का चौथा सबसे बड़ा सौन्दर्य बाजार भारत
27 Feb 2024

श्रणिका
27 Feb 2024
Jan Morcha for Communal Harmony in Bhopal
27 Feb 2024

Need To Protect Distinct Identity Of Uttarakhand
27 Feb 2024
Thought for the Day
26 Feb 2024



गाँधी जी का सामान
26 Feb 2024

न्याय यात्रा : असहज करती राहुल की अभिव्यक्ति
26 Feb 2024
Thought of the Day
26 Feb 2024



श्रणिकाऐ
23 Feb 2024
Thought for the Day
22 Feb 2024
अमीन सयानी की स्मृति : क्या थे वे दिन?
22 Feb 2024

इलेक्टोरल बॉन्ड के गोरखधंदे का पर्दाफाश
22 Feb 2024

श्रणिकाऐ
22 Feb 2024


Will Rahul’s Yatra convert into votes for INDIA
22 Feb 2024
Thought for the Day
21 Feb 2024

जब नेतागण जनता का धन और अपना हितसाधन करते हैं?
21 Feb 2024


श्रणिकाऐ
21 Feb 2024

Govt Takes Away More than Half of Our Earnings
21 Feb 2024

Thought for the Day
20 Feb 2024
किसान आंदोलन और स्वामीनाथन कमेटी
20 Feb 2024

श्रणिकाऐ
20 Feb 2024
Is Giving State Awards Really Desirable?
20 Feb 2024

MONOPOLY HOUSES FOR WHOM A CRISIS IS A CASH COW
19 Feb 2024
Thought for the Day
16 Feb 2024

श्रणिकाऐ
16 Feb 2024
चुनावी राजनीति के लिए एक और झूठ
16 Feb 2024

BJP gets 54 percent of electoral bonds
16 Feb 2024

बंदर की कलाबाजी
15 Feb 2024

रानियों का राजपाट!
15 Feb 2024



Thought for the Day
15 Feb 2024

बसन्त बनाम वेलेंटाइन डे !
14 Feb 2024

इश्क कीजे फिर समझिए, जिंदगी क्या चीज है...
14 Feb 2024

क्या बीजेपी-अकाली गठबंधन को मिलेगा नया जीवन?
14 Feb 2024


Thought for the Day
14 Feb 2024

विश्व खाद्य दिवस पर : पित्सा, पराठा और हम !
13 Feb 2024

Digital Media Can Counter Saffron Narrative
13 Feb 2024

Thought for the Day
13 Feb 2024
Thought for the Day
7 Feb 2024
Self-funded Rail budget earns profits
13 Feb 2024

पंजाब को पहला भारत रत्न कब मिलेगा?
13 Feb 2024
महंगा पड़ा संत कबीर का ज़िक्र
7 Feb 2024

बसन्त बनाम वेलेंटाइन डे !
7 Feb 2024
Thought for the Day
6 Feb 2024

PM’s Speech A Brave Talk And Morale Booster
6 Feb 2024


Thought for the Day
2 Feb 2024


Thought for the Day
1 Feb 2024



When do Hardcore Sports Spectators Stay Away
1 Feb 2024
Thought for the Day
31 Jan 2024


Nitish Kumar: Unworthy Son of Socialist Movement
31 Jan 2024

बजट : कृषि क्षेत्र के लिए प्रावधान की आवश्यकता
31 Jan 2024

एक बार फिर जाल फेंक रे मछेरे
31 Jan 2024
Thought for the Day
30 Jan 2024
लाइब्रेरी में ही क्लिंटन का इश्क जन्मा था !!
30 Jan 2024

समाजवादी आंदोलन के कपूत नीतीश कुमार
30 Jan 2024

FM Must Raise Funding For Farm Sector
30 Jan 2024

Double Speak a Hallmark of Saffron Party Leaders
29 Jan 2024
पच्चीस साल पहले, एक बेहद घृणित हत्या
29 Jan 2024

Thought for the Day
25 Jan 2024


Economic Prospects Of Ayodhya After Ram Temple
25 Jan 2024

विधानसभा चुनाव: संचार भाजपा की सफलता की कुंजी है
25 Jan 2024


Thought for the Day
24 Jan 2024
Lok Sabha Polls :Will Anti-Incumbency Hurt DMK
24 Jan 2024

The Right Course for Akhlesh Yadav
24 Jan 2024
अयोध्या की सरयू को उसकी पहचान दिलायी जाए
24 Jan 2024

मंदिर तो कांग्रेस का चुनावी नारा था
24 Jan 2024
Thought for the Day
23 Jan 2024

राम मंदिर : क्या अब धार्मिक विवाद थम जायेगा|
23 Jan 2024
Twenty-Five Years Ago, a Murder Most Foul
23 Jan 2024

Will Ram Mandir Get Modi Another Term ?
23 Jan 2024

राम मंदिर के बाद अयोध्या का आर्थिक परिदर्श
23 Jan 2024


Modi’s Rhetoric And Reality
22 Jan 2024

राम मंदिर : एक दृष्टिकोण यह भी
22 Jan 2024

भगवान राम के यह भक्त गायक
22 Jan 2024
Thought for the Day
19 Jan 2024
The Essence of Life Is To Be Happy
19 Jan 2024
WHAT DO LOK SABHA POLLS MEAN FOR SOUTH INDIA ?
19 Jan 2024


Thought for the Day
18 Jan 2024


Peter Magubane whose camera was his gun
18 Jan 2024
आपस मे लड़ती नहीं,पूजा और नमाज़
18 Jan 2024
डिकोड हुई सिंधु सभ्यता लिपि - उठा रहस्य से पर्दा
18 Jan 2024

युवा पीढ़ी और सिनेमा
18 Jan 2024
Thought for the Day
17 Jan 2024



हाइकु
17 Jan 2024

पुरानी बाते, कुछ यादे; पत्रकारिता तब और अब
17 Jan 2024
वर्ष 2023 और ईसाई समाज की विडंबना
17 Jan 2024
Thought for the Day
16 Jan 2024

क्या आने वाला बजट लीक से बिलकुल हट कर होगा ?
16 Jan 2024

खिचड़ी संक्रांति
16 Jan 2024

Is Ram Temple at Ayodhya a political project ?
16 Jan 2024
Thought for the Day
15 Jan 2024


अमेरिका में भारत-पाक की तरह की दलगत राजनीति
15 Jan 2024

कबतक , आखिर कब तक
15 Jan 2024

Ban Guns, Not Children
15 Jan 2024

New Budget May Have Certain Surprising Features
15 Jan 2024
Thought for the Day
12 Jan 2024

शीत लहर : बचाव और प्राथमिक चिकित्सा
12 Jan 2024

मेरी बात : मेरी व्यंग यात्रा और मेरे मित्र
12 Jan 2024


Thought for the Day
11 Jan 2024
Precautions And First Aid Tips In Cold Wave
11 Jan 2024


शेरिंग तोबगे: भूटान का भारत-मित्र प्रधानमंत्री
11 Jan 2024
Thought for the Day
10 Jan 2024

A good year for Bollywood
10 Jan 2024

राशिद खान जो गाते गाते जाने कहाँ चले गए
10 Jan 2024

नये साल मे देश की चुनावी राजनीति : एक आकलन
10 Jan 2024
Thought for the Day
9 Jan 2024

राम मंदिर: एक सच यह भी है।
9 Jan 2024

श्रणिकाऐ
9 Jan 2024


SC order in Bilkis Bano case hailed
9 Jan 2024
Thought for the Day
8 Jan 2024

अंतर्राष्ट्रीय हॉकी महासंघ का एक शानदार शतक
8 Jan 2024


Thought for the Day
5 Jan 2024
गायक मोहम्मद रफ़ी की स्मृति में भव्य स्मार्क
5 Jan 2024


Bhagwan Ram And Our Electoral Scenario.
5 Jan 2024
Thought for the Day
4 Jan 2024



U.S. Witnessing Indo-Pak Style Power Game
4 Jan 2024

Thought for the Day
3 Jan 2024

श्रणिकाऐ
3 Jan 2024
चुनाव का साल नया साल : नव वर्ष सभी को शुभ हो
3 Jan 2024

जन्मदिन की शुभकामनाए
3 Jan 2024


Happy New Year musings
3 Jan 2024

Thought of the day
2 Jan 2024

भारत की प्राचीन लोकतांत्रिक परम्पराए
2 Jan 2024

क्या मथुरा, काशी २०२४ में सुलझेगा?
2 Jan 2024

New Year : Indian politics at Cross-Roads
2 Jan 2024

Thought for the Day
29 Dec 2023
29 दिसंबर 1971 को एक इतिहास कैसे बना।
29 Dec 2023

AI can hit 70 polls, topple govts
29 Dec 2023


आज का सुविचार
28 Dec 2023

लोक सभा 2024 : चुनाव का वास्तविक महत्व
28 Dec 2023

हास्य से संसद जीवंत होता है
28 Dec 2023

25 Dec 1927 : The Day Manusmriti Was Burnt
28 Dec 2023

Thought for the Day
26 Dec 2023

Belittling the High Office
26 Dec 2023
Women welcome decriminalisation of Adultery !
26 Dec 2023

हिंदी साहित्य के सांताक्लॉज धर्मवीर भारती
26 Dec 2023

Thought for the Day
25 Dec 2023
25 दिसंबर 1927 मनुस्मृति दहन दिवस
25 Dec 2023
परीक्षा का बुखार
25 Dec 2023

OUR MEDIA IS LOSING INDEPENDENT FERVOUR
25 Dec 2023

उपराष्ट्रपति धनखड़ की राजनीतिक याञा
22 Dec 2023

विचार विमर्श
22 Dec 2023
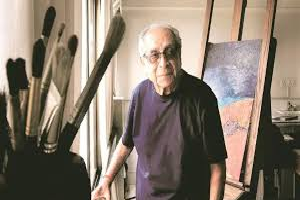
Delhi in the eyes of a young painter
22 Dec 2023
The lifeblood of Indian democracy
22 Dec 2023
Age shaming politicians
22 Dec 2023


श्रणिकाऐ
21 Dec 2023

सदन यदि संयम खो दे तो दिशाहीन होगी
21 Dec 2023

INDIA Alliance forges ahead crossing hurdles
21 Dec 2023

BJP after assembly elections
21 Dec 2023

विधान सभा चुनाव के बाद की भाजपा
21 Dec 2023

कोरोना काल में प्रतिरोधक क्षमता कैसे बढ़ाए
20 Dec 2023
Plight Of Unorganized Workers
20 Dec 2023
पुष्पा भाभी को व्यास सम्मान
19 Dec 2023

मार्गदर्शक या मार्गकंटक?
19 Dec 2023

श्रणिकाऐ
19 Dec 2023

Our Real But Unlisted Minority
19 Dec 2023
West Asia: European dominance coming to an end
19 Dec 2023



श्रणिकाऐ
18 Dec 2023

CAN RISK GLOBAL BIZ
18 Dec 2023

असंगठित कामगारों की व्यथा
15 Dec 2023

ऑफ द रिकॉर्ड पत्रकारिता के खतरे !
15 Dec 2023
आपस मे लड़ती नहीं,पूजा और नमाज़
15 Dec 2023

Afghan Tragedy Unfolds in Pakistan
15 Dec 2023

Meaning of Modi-Shah’s Choice of three CMs?
15 Dec 2023


मेरा नाम सिंह है और मैं आतंकवादी नहीं हूं
14 Dec 2023


My name is Singh and I am not a terrorist
14 Dec 2023

वित्त मंत्री निर्मला सीतारमण
13 Dec 2023

हास्य व्यंग्य
13 Dec 2023

कश्मीर पर सुप्रीम कोर्ट
13 Dec 2023
The Seasonal Disease Of Examination Fever
13 Dec 2023
Human Rights Day
13 Dec 2023

मानवाधिकार दिवस : 10 दिसंबर
12 Dec 2023
राजधानी
12 Dec 2023

She's protesting too much
12 Dec 2023


मिजोरम और छत्तीसगढ़ के चुनाव परिणाम
11 Dec 2023

राजस्थान में कांग्रेस क्यों हारी?
11 Dec 2023


Securing Data The Most Valuable World Resource
11 Dec 2023
बिगड़े हैं तेवर नगर के !
8 Dec 2023

अंबेडकर और मार्क्सवाद
8 Dec 2023
Without moon
8 Dec 2023


दिल्ली का द्वार !
7 Dec 2023

मजदूर वर्ग हित और संसदीय प्रणाली
7 Dec 2023


INDIA block for whom?
7 Dec 2023


त्योहारों का देश !
6 Dec 2023

चाहे हेड पड़े, या फिर टेल
5 Dec 2023

मानसिक तनाव से मुक्ति पाए
5 Dec 2023

A DIFFERENT WAY TO MEET
5 Dec 2023

Time for some heads to roll in Home Ministry
5 Dec 2023

शिक्षा, विकास और नास्तिकता का परस्पर संबंध
4 Dec 2023
आप सन्त नहीं,महंत नहीं,सिर्फ एक दुकान हैं !
4 Dec 2023

Media and Crisis of Credibility
4 Dec 2023

भारत माता -एक विमर्श
1 Dec 2023

संकट में लंदन का डेली टेलीग्राफ
1 Dec 2023


Ladakh to Manipur – billions lost
1 Dec 2023

पाकिस्तान में अस्था का संकट
30 Nov 2023

न्यायिक व्यवस्था मे सुधार
30 Nov 2023

Assembly Pools: Will Telangana throw a surprise.
30 Nov 2023

Travel from Canada to India in Troubled Time
30 Nov 2023
STATE POLLS
29 Nov 2023

साक्षात्कार
29 Nov 2023

Humour
29 Nov 2023

क्या अब भाजपा मुक्त दक्षिण भारत होगा ?
29 Nov 2023

एशिया पेसेफिक इकनॉमिक को-ऑप्रेशन का पैग़ाम
28 Nov 2023

दलित सबलीकरण : मीडिया की भूमिका कितनी अहम
28 Nov 2023

A BJP-mukt South India on December 3?
28 Nov 2023

Naushad khan's interview of Pradeep Mathur
28 Nov 2023

Netanyahu’s Pride Humbled
27 Nov 2023

Remembering Mrs Indira Gandhi
27 Nov 2023

चार्ल्स ने शहीदों से माफी मांगी !
27 Nov 2023

नज़्म गजह (गाज़ा)
27 Nov 2023


राजनीतिक विमर्श के गिरते मानक
25 Nov 2023
Amit Shah: Ignorance, dogma, and prejudice
25 Nov 2023
Bengal rockets to sixth rank
24 Nov 2023

भारत के बुरे दिनों में मित्र रहे जॉन कैनेडी !
24 Nov 2023

तेलंगाना विधानसभा चुनाव और ओवैसी की राजनीति
23 Nov 2023


Deteriorating standards of political discourse
23 Nov 2023

दिवाली पर रिकॉर्ड बिक्री, बचत में कटौती
23 Nov 2023

Current Issues Education
22 Nov 2023

भारतीयता की परिभाषा
22 Nov 2023

भारत-मित्र हैं तो चीन के शत्रु भी !
22 Nov 2023
On National Press Day Observed Last Week
21 Nov 2023
Diwali sales a record, cut savings
21 Nov 2023
19 नवंबर: जन्मदिन पर श्रद्धांजलि
21 Nov 2023

Nov 19: A Birthday Tribute
20 Nov 2023

सिंधी व्यापारी का लंदन होटल है!
20 Nov 2023
THE IDEA OF INDIA
20 Nov 2023

हास्य व्यंग्य
20 Nov 2023
आज तुम उदास होओगे
14 Nov 2023
जब जब नेहरू का जिक्र आता है
14 Nov 2023
Nov 14 : Nehru’s Birth Anniversary
14 Nov 2023



खड़गे एक सफल और सक्षम कांग्रेस अध्यक्ष
3 Nov 2023

Has Congress found a leader in Kharge?
2 Nov 2023


RAISING COSTS TO CUT POLLUTION!
28 Oct 2023

महुआ मोइत्रा की ज़बाँबन्दी और महिला आरक्षण
26 Oct 2023

The World is at War?? Is it the Karmic Cycle of
26 Oct 2023

relationship between Samajwadi Party Congress
26 Oct 2023


रावण का पुतला लगता है उदास
25 Oct 2023

क्या भूलूं ...? क्या याद करूं ?
25 Oct 2023

जो नहीं हुआ २० साल से विराट ने कल कर दिखाया
23 Oct 2023

इज़्राईल और फ़िलस्तीन : जंग का रंग बदलने लगा
23 Oct 2023